
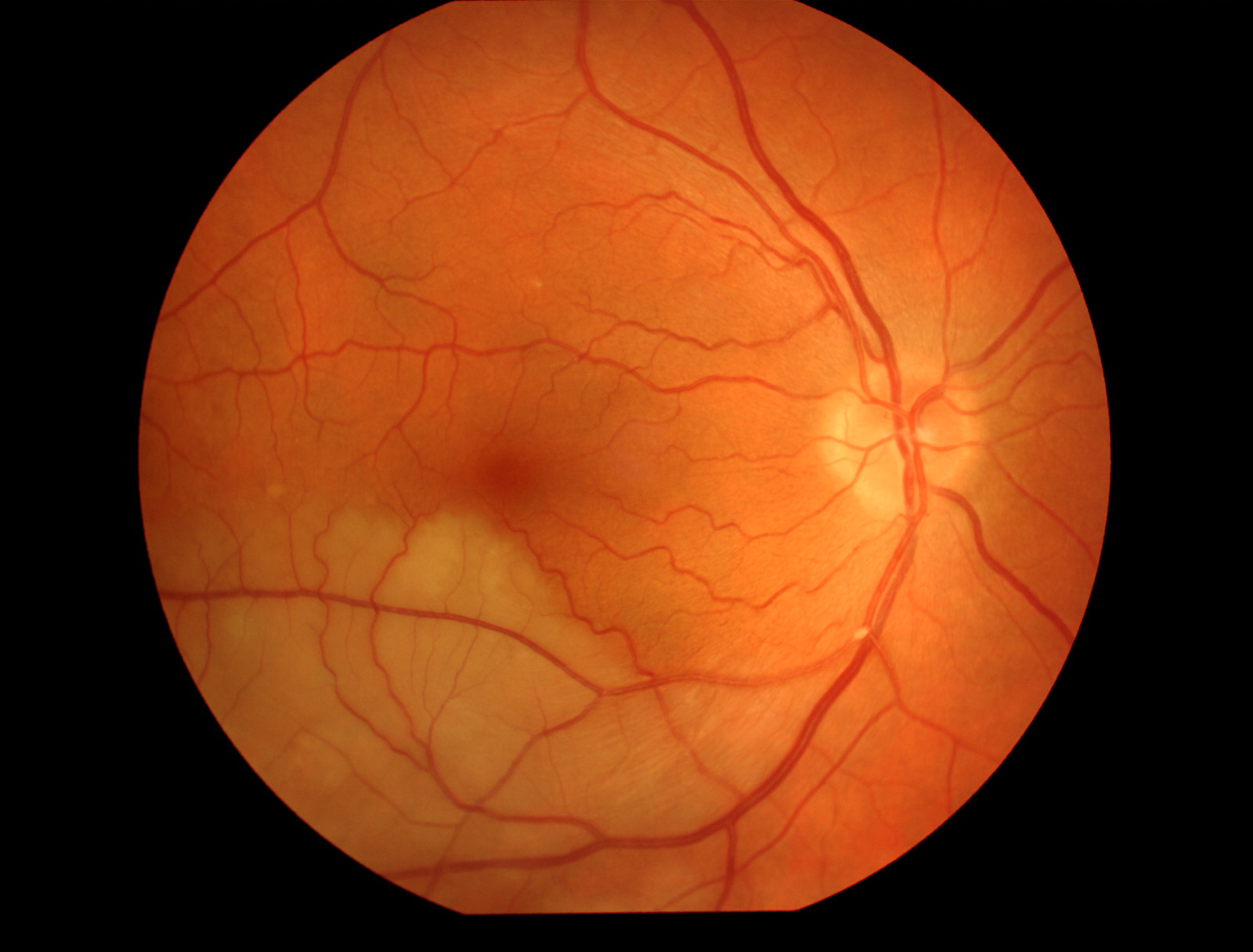
Kristen Wagner, COT, OSC. Branch Retinal Artery Occlusion; Retina Image Bank; Year: 2019; Image Number: 42542

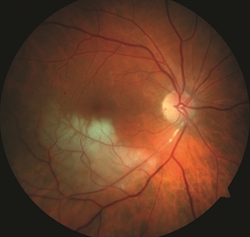
Hyung-Woo Kwak, MD. Central retinal Artery Occlusion; Retina Image Bank; Year 2012; Image Number 1683

Mehul A. Shah, MD. Retina Image Bank 2014; Image 19815. ©American Society of Retina Specialists.
John S. King, MD. Retina Image Bank 2014; Image 18552. ©American Society of Retina Specialists.

Courtney Crawford, MD. Retina Image Bank 2017; Image 26792. ©American Society of Retina Specialists.

